

Best Practice Medical Treatment Pays Huge Dividends in Heart Artery Disease
Best Practice Medical Treatment Pays Huge Dividends in Heart Artery Disease
The Promise of Optimal Medical Therapy (OMT)


When I started this site Jan 1, 2021, most of you were not aware of it. I started with the highest risk, most costly conditions first. This is where optimal medical treatment can have the most impact.
Heart disease is the leading cause of death in the United States. One in every four of us will die of that condition. One fourth of heart attack patients have no risk factor identified prior to the event and so there is no warning. Male sex and age are major risk factors. Therefore, a sixty-one-year-old man has a cardiac risk estimate of 7.9% in the next ten years. Nearly 8% of those men will have a heart attack in the next decade. His age and sex alone make him high enough risk to recommend statin treatment and blood pressure control to 130 on the top number. Use the cardiac risk link to calculate your own likelihood of having a heart attack.
The person who has already had a heart attack is especially high risk for dying or having another heart attack. Surveys show that 13% of Medicare patients have already had a heart attack and another 12% have heart artery disease. Patients who receive usual care with heart disease—the care that most of us receive—are especially high risk when compared with those who benefit from best practice treatments or optimal medical therapy (OMT).
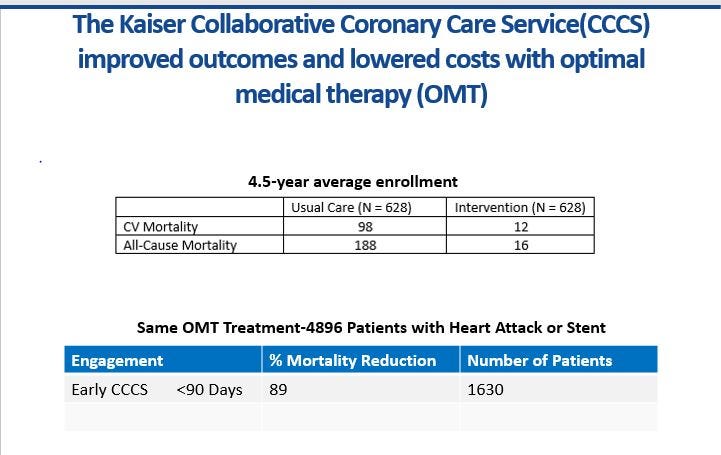
The most important medical study of heart attack patients in the last 50 years came from the Kaiser Permanente organization in Colorado. They compared 628 heart attack patients receiving usual care with 628 individuals assigned to a team of nurses and pharmacists who made certain they got every element of best practice treatment or OMT. The team worked diligently to assure that every OMT patient achieved their cholesterol, sugar, and blood pressure goals while stopping smoking and taking aspirin. They performed much better than usual care. The average LDL cholesterol was 78 and the average blood pressure was 126/72. 99% of patients were taking aspirin or another anticoagulant. 91% were on a statin. 93% of those with diabetes were on a medication like lisinopril or another generic medication ending in -pril. You can see easily that OMT for heart attack victims includes aggressive targets for blood pressure, cholesterol, and sugar, along with stopping smoking and taking aspirin.
The results of OMT are very dramatic. If you have a heart attack, and you receive OMT you are ten times as likely to live to see your grandchild graduate or get married 5 years later. Patients who received OMT also cost $21,900 a year less than usual care patients because they did not go into the hospital as often with additional heart attacks, extra beats, and heart failure. Today we can do even better. Patients who have had a heart attack should achieve a blood pressure of 130/80 or less, a glucose of 100 or less (HbA1c of 7), and an LDL of 70 or less while stopping smoking and taking aspirin. The treatments used to achieve those goals are equally important and we can talk more about that tomorrow. The path to better health at lower cost in patients who have had a heart attack is very specific and the results are proven. That is what we should do until someone shows better results.