

Care for Congestive Heart Failure is Still Awful
Care for Congestive Heart Failure is Still Awful
But You Could Do Something About It

Congestive heart failure is still a huge source of cost, disability, and death, especially in the Medicare population where eleven percent of beneficiaries are affected. A Milliman analysis says that heart failure patients account for 34% of all Medicare spending and 55% of Medicare fee-for-service readmissions. These patients cost $3482 per patient per month which is almost $42,000 per year. Most of those costs are related to hospitalizations. Medical research and the tools to improve health and lower cost in heart failure are making great strides, but because we don’t apply them , the number of cases and costs continue to increase.
Heart failure is not just one disease, but at least two. Patients with heart failure and a low pumping capacity are the ones we can help the most. The heart normally ejects 60% of the blood it contains with each stroke. The answers for patients that eject 40% or less are very well worked out. Patients in the 41-50% range respond to those same measures, and those over 50% have a different disease and don’t respond as well.
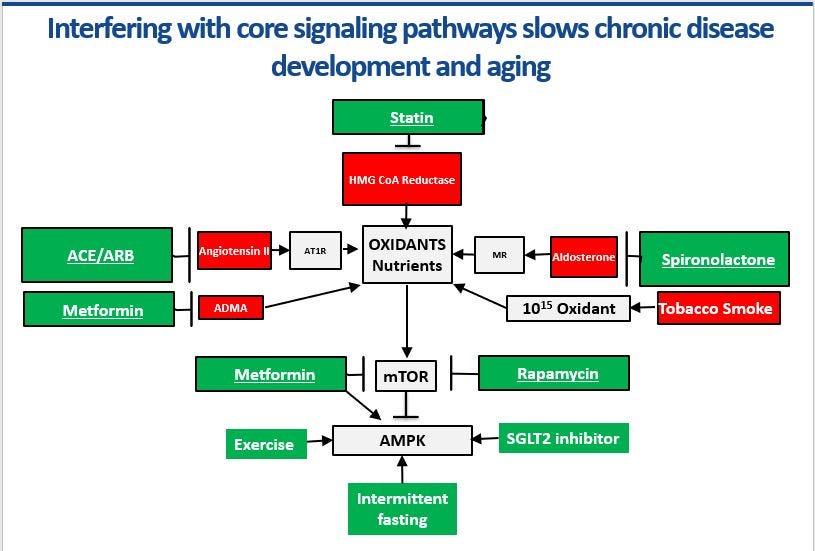
Heart failure patients with a pumping function of 50% or less should be on adequate doses of an ACE inhibitor (lisinopril) or an ARB (losartan), a beta blocker (carvedilol), and an MR blocker like spironolactone or eplerenone. There are mountains of evidence supporting these treatments as disease modifying therapies. Spironolactone alone reduces the likelihood of hospital admission by about a third, but only a third of these patients are taking it. SGLT2 inhibitors like Jardiance do the same thing, but it is fairly new, expensive and not often used for heart failure.
A new study from the Journal of the American Medical Association reviewed care for these patients in the Veterans Administration. β-blocker (carvedilol) use was 72.0% and spironolactone or eplerenone use was just 27%. Rates for angiotensin receptor-neprilysin inhibitor therapy were at 22%. Just based on B-blocker and eplerenone use, only about 19% of these patients are getting the treatment they should receive for this exceptionally high-risk, high-cost condition. Most of the patients not on these medication do not have an intolerance, allergy, or contraindication. It is a systems problem.
So, what is to be done? A cardiometabolic advanced medical home team can take on heart failure along with their other targeted cardiovascular conditions. First, heart failure patients must be segmented into low and normal pumping function diagnostic codes. That is critical to close gaps and follow outcomes at a population level. That can be handled based on their echocardiogram. If they have not had one, get one. Put a diagnosis in the chart that reflects their pump function status. If they have low pump function, they should be on adequate doses of ACE/ARB, B-blocker, and spironolactone/eplerenone. Those three medications can be added for $12 per month. It they are still having symptoms and hospitalizations, add empagliflozin (Jardiance $550/mo). That is an expensive medicine but one day in the hospital easily buys a year’s supply. If you are a heart failure patient, you can be much safer. If you take care of heart failure patients, it is not that hard to keep them out of the hospital, improve their health, and save money. Let’s get started!
The saddest part of the late stage sickness seeking American medicine is the horrific consequences and carnage inflicted on the heart failure patients. Ignoring early detection, early warning, primary prevention measures to treat the root causes of heart failure, the system has failed completely as result of pursuing profits instead of improving patients chances of NOT developing heart failure in the first place. The cardiology community has the collective responsibility to acknowledge this moral failure, professional negligence, beg God and the poor suffering patients for repentance, and forgiveness. Time to fix the system.