


Drug Company Money and Our Dysfunctional Healthcare System
They Don’t Serve You


My last post was about the pernicious effect of direct-to-consumer drug advertising on healthcare costs and results. The medical information provided by professional organizations like the American College of Cardiology is distorted by the same forces. There is an unholy alliance between big pharma, leading American academic institutions, and professional organizations.
The Coordinate-Diabetes Study was just presented with great fanfare at the annual sessions of the American College of Cardiology. This trial was a study of best practice interventions by cardiology departments in patients with type 2 diabetes and atherosclerotic vascular disease. These are very high-risk patients. Powerful statins, ACE inhibitors like lisinopril, ARBs like losartan, SGLT2 inhibitors like Jardiance or Farxiga, and GLP-1 drugs like Trulicity are proven to reduce heart attacks and strokes for patients with vascular disease and type 2 diabetes. The study was designed and conducted by the Duke Clinical Research Institute. It is the largest academic clinical research institute in the world. This academic research institute has a partnership with Novo Nordisk and other diabetes companies. Here is a list of the ways the research institute gets money. Funding for the study was provided by Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI) and Lilly USA, LLC. Boehringer Ingelheim and Eli Lilly make the SGLT2 inhibitor Jardiance. Boehringer is developing a GLP-1 drug as well. Eli Lilly makes the GLP-1 drug Mounjaro.
The purpose of the study was to increase the percentage of patients taking the above classes of diabetes medication in the study group vs. the usual care group. These three treatments were prescribed together in 15% of usual care patients and 38% of the intervention group. So, the intervention had some improvement effect.
The researchers looked at the difference in clinical events between the intervention group and the usual care group. Clinical events are the most important information from this study. Patients with type 2 diabetes don’t die of high sugar. They die of heart attacks, strokes, and heart failure. The impact of this study was very modest. There was a 1.8% real difference in the number of patients who had one of these serious events.

The impact of this study on best practice medicines is modest as well except for doubling the use of the medications produced by the drug companies that sponsored the research.

There was no significant change in risk factor levels.

As stated before, Boehringer Ingelheim and Eli Lilly make the SGLT2 inhibitor Jardiance. Boehringer is developing a GLP-1 drug as well. Eli Lilly makes the GLP-1 drug Mounjaro. The cash price of Jardiance is $700 a month or $8400 a year. The cash price of Mounjaro is about $1200 a month or $14,400 per year. “People with diagnosed diabetes incur average medical expenditures of $16,752 per year, of which about $9,601 is attributed to diabetes. On average, people with diagnosed diabetes have medical expenditures approximately 2.3 times higher than what expenditures would be in the absence of diabetes.” When a clinician prescribes Mounjaro, that doubles the costs for diabetes care for your self-insured health plan. About 10% of adult Americans have type 2 diabetes. If there are 5000 adult members in your health plan, there would be 500 diabetics. Prescribing Mounjaro for these patients would increase your healthcare spending by over $7 million. Those are the solutions you get from a healthcare system riddled by conflicts of interest.
This study is designed to convince prescribers to use these very expensive drugs in preference to proven protocols that use generic medications like metformin. It only lasted a year. It produced very little difference in important clinical outcomes. It was supported by drug companies that make these diabetic drugs. Drug companies answer to their stockholders and executives and that is who they serve. They don’t answer to you. They don’t serve you. It is to be expected that they would sponsor research that makes their products look good.
Here is the great news! There is a much better answer to the problem of high-risk diabetes. The study above is not a real best practice or optimal medical therapy (OMT). Best practice protocols doesn’t just look at lisinopril or losartan for high blood pressure, a statin for cholesterol, and a medication for diabetes. It also requires aspirin treatment for high-risk patients and nonsmoking patient status. It also requires achieving a blood pressure of 140/90 or less and an A1c of 8 or less. Had those elements been included, their performance of OMT would have been even worse.
Let’s look at an optimal medical therapy or best practice trial for patients with high-risk diabetes done in a diabetes clinic Europe and started in 1995. As with the study above, this trial looked at the impact of OMT on a collection of cardiovascular events. including death from cardiovascular causes, nonfatal heart attack, nonfatal stroke, bypasses, stents, and amputation. This European study (Steno 2) had a much greater impact on risk factor levels. Patients in more intensive treatment had a top number on their blood pressure that was reduced 14 points from the beginning of the study and 11 points compared with usual care. LDL or bad cholesterol was reduced 47 points from baseline and 34 points compared with usual care. Patients in intensive treatment had about half as many cardiovascular events as usual care patients. That is a huge difference compared with the 1.8% difference in the study above.
This European study after 5 more years showed even more dramatic differences at 13 total years of follow-up.
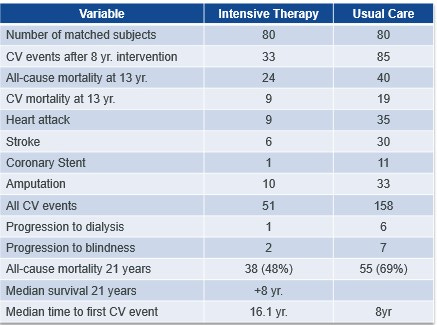
Notice that the improvements at 13 years of follow-up were not 1.8%. Optimal medical therapy patients had one third as many cardiovascular events as people in usual care. At 21 years of follow-up, the intensive therapy patients lived 8 years longer free of heart attacks and strokes compared with patient in usual care. There was a 70% reduction in hospital admissions for congestive heart failure.
The diabetes medicine used in the European study was metformin. Now you may think that Jardiance is a better drug than metformin, since metformin has been in use for 50 years, but it is not. Jardiance and metformin both switch on the master genetic metabolic survival switch AMPK which protects all cells and organs whether the patient is diabetic or not. The huge difference is cost and profit. The cash price for Jardiance is $700 a month. The cash price for metformin is $4 a month. Jardiance costs 175 times what metformin costs.
The European and American diabetes guidelines both recommend metformin as the first choice drug and the Coordinate-Diabetes Study does nothing to change that. We agree that a medication like Jardiance makes sense as the next drug if the sugar or risk remains too high. We help practices with the systems and protocols to provide optimal medical therapy consistently. This approach is proven to work. One of our clients has lowered the total cost of care by half while reducing ER visits by 2/3 and hospitalizations by 80%. I am confident they will do better still as we refine our processes. You need to get your clinical information from sources without conflicts of interest.
I don't think you realize the peer-reviewed journals are corrupted also. If you actually read the studies, many of them argue for the repurposed drugs, even though their headline and abstract was negative. Many were set up to fail using dangerously high doses or choosing patients far too late into the sickness. You have to actually read each paper to see the corruption. The censorship of very good studies is breathtaking and so depressing. I have read countless papers that have come out both pro and con. The evidence is overwhelming In favor of using effective repurpose drugs along with solid protocols. See for instance flccc.net excellent protocols . Around the world many countries use similar early treatment protocols, but the US with the highest covid deathrate remains stiff necked and blind.
Among others, the FLCCC also provide wonderful analysis of the big papers as they came out, both " peer reviewed" and censored. I am a peer reviewer for scientific papers so I know how to read them. It is tragic how many unnecessary deaths there were. The corruption is complete throughout the medical industry. I battled it personally 20 years ago when my eyes were opened about statins and niacin. Sadly it's the same across the board. If you have only read mainstream medical papers, then you are correct, you have not seen much evidence and you also did not critically assess the methods in those papers. I cannot help you on that. But you need to read all the papers and talk to the real doctors who treated hundreds and thousands of patients using effective early treatment protocols. Their patients did not get long COVID and did not die. Early treatment must be started as soon as symptoms appear. Prophylactic protocols also are extremely effective.
Completely agree. Pharma has taken over medicine, corrupting the doctors and healthcare, completely forgetting the patients. Push more and more $$$ expensive drugs. The covid fiasco put it all on center stage as the medical cartel preferred seeing people die rather than recommending early treatment with repurposed very effective drugs to stop the virus in its tracks. It is shameful and in every sector. The diabetes study is just more of the same. So sad for trusting consumers who do not know better. Sad state of affairs.