

Hard Proof You Can’t Reverse Type 2 Diabetes
Hard Proof You Can’t Reverse Type 2 Diabetes

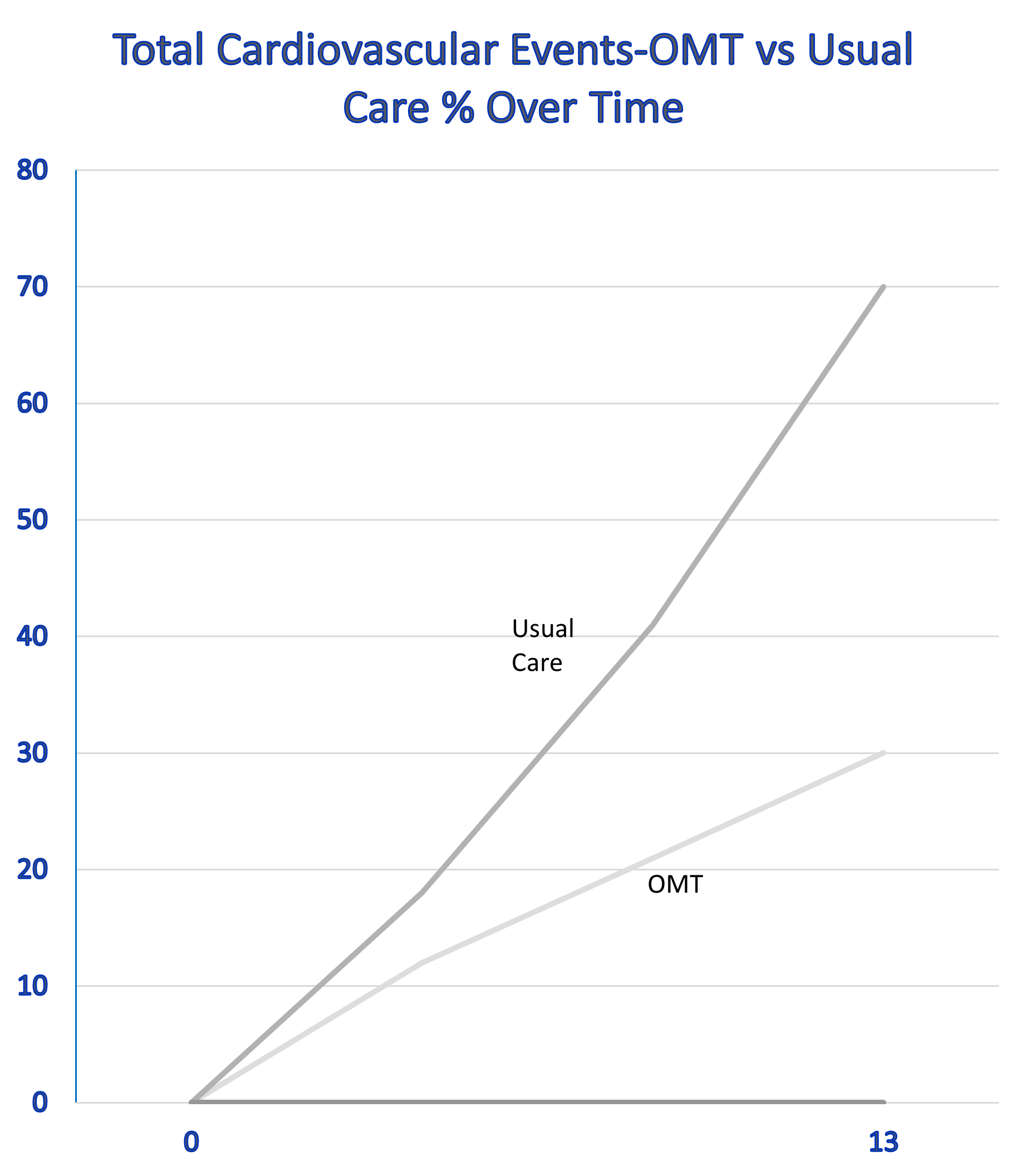
The last post reviewed evidence that you cannot reverse type 2 diabetes. This post will produce hard proof. I have worn you out with the very impressive results of optimal medical therapy (OMT) for type 2 diabetes when compared with usual care— the care that most of us receive. This graph compares death from cardiovascular causes, nonfatal stroke, nonfatal heart attack, coronary-artery bypass grafting (CABG), stents for heart artery blockage, other surgery to open atherosclerotic arteries, and lower leg amputation in patients on optimal medical therapy (OMT) vs usual care over a 13 year period. You can easily see there is a huge difference in these important outcomes.
Notice that these were very high-risk patients with type 2 diabetes and chronic kidney disease. By 13 years, 70% of the usual care patients had had one of these events compared with only about 30% of the OMT patients. If you review the paper in the link, 13 years into the study, fully half of the usual care people were dead. Patients entering the study had type 2 diabetes with chronic kidney disease and the average age of participants was 55. Again, half of the patients in usual care were dead by age 68.
There is now 21 years of follow-up for this study and these huge difference in outcomes have persisted. Here is the most remarkable fact about this entire study and it proves beyond a doubt that you cannot reverse diabetes. There was an intermediate analysis done 7.8 years into the study. Even then, the individuals in the OMT group had a risk of the above cardiovascular outcomes that was less than half. To their everlasting credit, the investigators running the study decided that it would be unethical to continue the usual care arm of the study. At that point, every patient in the study went on OMT. Just to be perfectly clear, from 8 years on out, all patients in the study were on OMT. You would expect the outcomes graph to come closer together after eight years, but that did not happen. Despite the fact that all patients were on OMT going forward, the patients who were on OMT early continued to do much better than the usual care patients. Both links go to papers in the New England Journal of Medicine which is one of the half dozen most reputable medical periodicals.
This result is completely baffling under our current scientific paradigm that depends on lowering the sugar level to reduce diabetes outcomes. Lowering the sugar alone will never produce outcomes that are equivalent to lowering the blood pressure, cholesterol, and sugar while stopping smoking and taking an aspirin if very high risk as these patients were. OMT in diabetes is defined by accomplishing these five goals concurrently while using diet and exercise along with losartan or lisinopril for blood pressure, a statin for cholesterol, and metformin for diabetes.
The result makes perfect sense if you understand gene regulation (epigenetics) and how that relates to “metabolic memory.” As in the study we are currently reviewing, multiple clinical trials have underscored the long-lasting beneficial effects of more aggressive treatment on the serious complications of diabetes. They have also demonstrated that diabetic complications such as diabetic kidney disease can continue even after blood glucose normalization, suggesting a metabolic memory of the prior glycemic state.
This epigenetic science is the new frontier of aging and chronic disease science. It is the science of gene regulation. As you know, DNA is the bit of computer code in a gene that produces its effects. Epigenetics determines which bits of computer code is active and which are not. Ordinarily, DNA is tightly wound and inactive. Epigenetic works by chemical changes in the DNA that open it up so that the code can be read. These epigenetic changes in diabetes are long lasting. That can be inherited and passed on to the next two generations. “….studies in vascular cells have shown long lasting changes in epigenetic modifications at key inflammatory gene promoters after prior exposure to diabetic conditions suggesting a possible mechanism for metabolic memory.”
This diagram below shows how these epigenetic changes work. These genes that are inappropriately turned on lead to increased oxidant production and that causes inflammation, increased scar tissue growth, and the death of functional cells in the kidney, heart, and liver that cause organ failure.
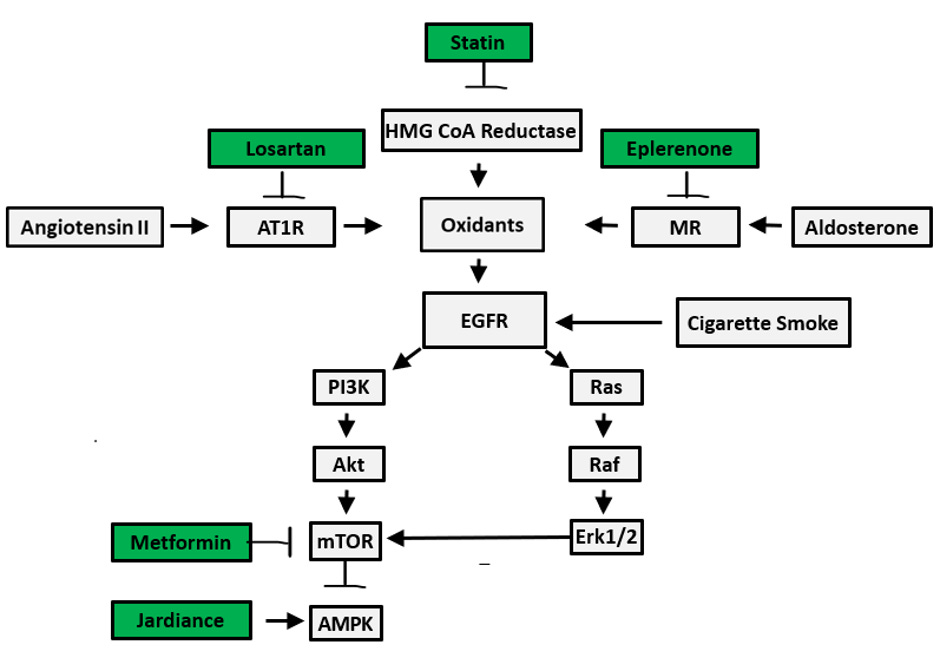
The medications in the green boxes interfere directly with these epigenetic changes that I have described to dramatically reduce all diabetes complications. Drastically reducing carbs and sugar to get your blood sugar down below diabetic levels is a great thing. It is important. But it does not reduce your risk to that of a normal person. Nothing will reduce your risk to that of a normal person that was never diabetic because your genes are now changed. You have genes that are switched on that will stay switched on. To block the effects of those genes you must be on the medications in the green boxes. If you do that, you will be one fourth as likely to have a heart attack, one fifth as likely to have a stroke and you will live eight years longer compared to patients in usual care— the care that most of us receive. I wish you could reverse diabetes. This is hard proof that you can’t. You can have much better health at lower cost with optimal medical therapy and that is the model we must scale as rapidly as possible. It is still unethical to not provide best practice treatment to all patients. Help us make certain that optimal medical therapy is available to everyone.
The question is since we know that T2D is irreversible, why would we keep pushing treatments that are not cures?
The next question is these drugs target bits of pieces of a partially understood roadmap of an extremely complex biological system, how can we declare victory over these partial and incomplete treatments as the best thing next to a slice of bread?!?
The issue I have with the legacy 19th Century Analog Medicine is its systematic failure to address the fundamental understanding of the root causes of chronic diseases and finding the cures we all deserve. Instead, the entire system focuses on the “late-stage-sickness-profiteering” with no cure insight.
Time to throw out the old corrupt box and build a new one, Bill.
We are doing it, and are making headways!
Thankfully.
Cellular aging, T2D, cancer, cardiovascular and cerebra-vascular diseases have one thing in common, metabolic dysfunction making cells vulnerable to diseases.