

How An Oncologist Would Treat Her Own Melanoma
How An Oncologist Would Treat Her Own Melanoma

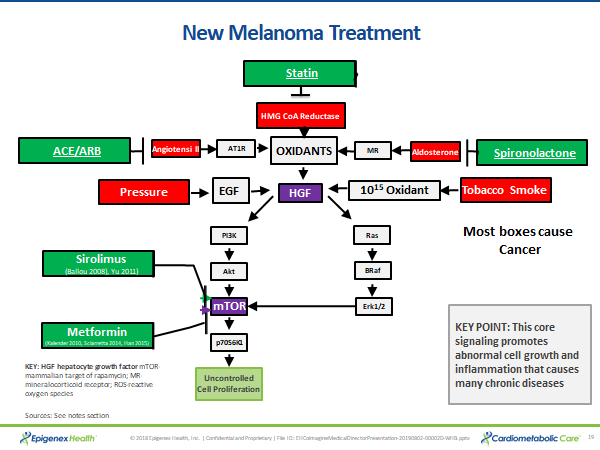
This link goes to an article from the director of the malignant melanoma program at the Cleveland Clinic on how she would want to treat her cancer if she had melanoma herself. She starts off very optimistically, saying that the science of melanoma is advancing quickly, and we are seeing longer survivals from this aggressive tumor as a consequence. The first test she mentioned is for BRaf mutation. That is a common mutation in melanoma. I put a similar diagram on each post, but this one shows more detail. BRaf is in the lower right corner of the diagram. When it is constantly switched on due to this mutation, it constantly switches on mTOR and switches off AMPK to support wild tumor growth. There are small molecule inhibitors against BRaf available for treatment.
The diagram provides another major insight into the cause of melanoma. In my other posts, the epidermal growth factor receptor (EGFR) is in the purple, central position. There are four different EGFR types, and EGFR2 (HER2) is persistently switched on in breast cancer. In melanoma, hepatocyte growth factor (HGF) is persistently switched on and drives tumor growth. Growth factors in general play a central role in cancer and vary according to the tissue and tumor type involved. Any one of these growth factors can be substituted in the central purple box.
The current treatment for melanoma with the best results is combination immunotherapy. There are exciting trials of new treatments that target the immune system. This expert recommends that as a first step and thinks these trials offer great promise. Here is the major takeaway. Hundreds of basic scientists have been working on the biology of cancer and there are precision treatments available today. There is every reason to be hopeful even with the most dangerous tumors. This is another powerful example of the ways in which aging, cancer, artery, and metabolic diseases are related. That fact has important implications.
Optimal medical therapy (OMT) first is the new standard of care for patients with stable heart artery disease. In a ten-year follow-up of these patients, fewer than half were on OMT. That is a real tragedy because at 10 years twice as many of those not on OMT were dead of all causes. Said another way, OMT cuts all-cause mortality in half. You can live a longer, healthier life now.