

Jean Had Repeated Chest Pain, No Heart Artery Blockages, and Global Cardiac Ischemia. (Poor Blood Supply to the Whole Heart) What??
Jean Had Repeated Chest Pain, No Heart Artery Blockages, and Global Cardiac Ischemia. (Poor Blood Supply to the Whole Heart) What??

Yesterday’s post discussed my neighbor Jean and her repeated chest pain. Her multifunction cardiogram (MCG) showed “global ischemia.” That means blood flow in the entire heart is reduced. Since this new technology is so new, I had a few respected colleagues review to article to make sure it all ties together. One of them asked, “If her heart cath was completely normal, how could she have global ischemic.” Of course, that is a key question, and here is a great article on the topic.
When women have repeated chest pain, our entire healthcare system focuses on the large arteries on the surface of the heart. We do a stress test, if there are changes indicating poor blood flow, then we do a heart catheterization, and if there is no blockage of one of these large surface arteries, then there is no heart artery disease. The stress test is deemed a “false positive”, the cardiologist says her heart is fine, she need not see him anymore, and she can stop aspirin. But she could only last two minutes on a treadmill, and her MCG showed global ischemia. How do you reconcile that?
These women have coronary microvascular disease (CMD). That is disease of the small vessels between the large arteries on the surface and the tiny capillaries that are the smallest vessels of all. Their entire heart circulation is involved. Therefore, blood flow to the whole heart is reduced—thus global ischemia. Women with repeated chest pain have a high risk of heart attack in the absence of chronic blockages of the large arteries on the surface of the heart. The have CMD, but they also have diffuse cholesterol plaque deposits throughout their large arteries that don’t block the artery. These plaques may rupture or erode, initiating the clotting process, and acutely blocking a large surface artery, causing a heart attack. The CMD increases the flow impairment and increases the likelihood of heart attack. Men tend to have heart disease characterized by more fixed blockages. Women have fewer fixed blockages, and more CMD. I had local disease. Jean had disease impacting the entire heart.
These changes in understanding how women have heart attacks has led to a transformation in the way heart artery disease is defined. Before, if a patient had a blocked surface artery identified with imaging, risk factor management was called “secondary prevention.” If there were no blockages or history of heart attack or stroke, efforts to reduce risk were labeled “primary prevention.” Now we know that albumin in the urine or decreasing kidney function means there is microvascular disease in that organ. In fact, as kidney function declines, CMD increases. Microvascular disease in the eye of a patient with diabetes poses a risk to vision and means the patients with diabetic eye disease is much more likely to have CMD.
Coronary microvascular dysfunction (CMD) is common in women with no large heart artery blockages and repeated chest pain. That term applies to the small vessels between the big arteries on the heart surface and the capillaries. It impacts the entire heart.
Here is more analysis from the landmark WISE study (Women’s Ischemic Syndrome Evaluation) funded by our own National Institutes of Health and executed by some of the best medical institutions in the country. There are 4 million Americans with this condition. If you see older patients, they are common in your practice. Diabetic women with CMD also have chronic kidney disease and eye damage. These are all microvascular conditions. Diabetic neuropathy is microvascular. So are strokes, dementia, and diabetic foot ulcer.
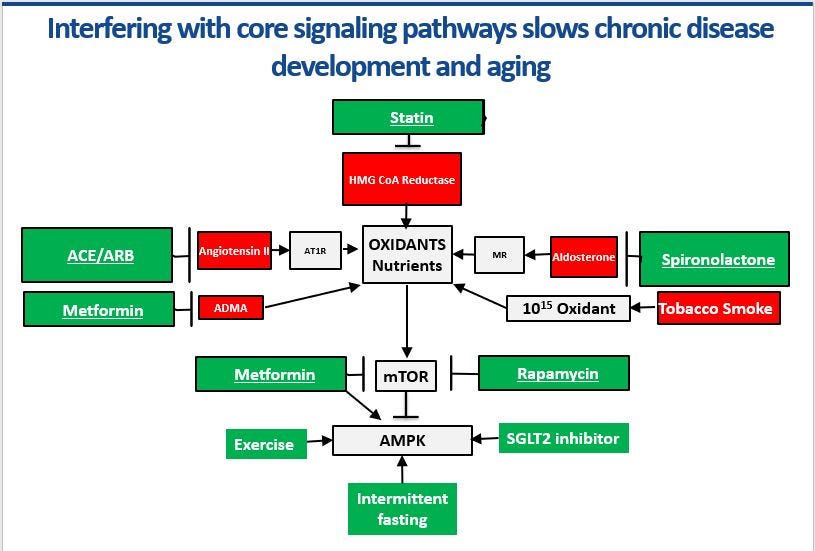
CMD’s cause is multifactorial. Women with extra abdominal weight, diabetes, hypertension, high cholesterol, elevated triglycerides, low HDL cholesterol, and a smoking history are more likely to be affected. Therefore, the treatment must be multifactorial. Optimal medical therapy (OMT) is a comprehensive solution that combines best practice diet, exercise, and molecular medical management supported by primary care teams focused on chronic disease, using population health tools, and protocols, while incentivized by a value-based payment model. Hard proof exists that this approach works in microvascular arterial disease. Remember—chronic kidney disease is a microvascular condition. As kidney function falls, heart attack risk goes up. Patients with type 2 diabetes and chronic kidney disease have one fourth as many heart attacks, one fifth as many strokes, one sixth as many go on dialysis, and one third as many lose their vision compared with usual care. Microvascular disease requires molecular medical management (MMM) In patients with known heart artery disease, OMT lowers mortality by 76% while saving $21,900 per patient per year compared with usual care. These great results are because OMT has very favorable effects on microvascular disease. Every green box intervention in the diagram above increases nitric oxide production in these small arteries.
Dr. Milton Packer is one of the most famous cardiologists in the country. Here he is writing about a diabetes drug in a diabetes journal on its impact on heart failure and chronic kidney disease: “it is now critical for physicians to reconceptualize SGLT2 inhibitors as organ-protective agents rather than glucose-lowering drugs. The antihyperglycemic action of these drugs represents a tiny fraction of their broad portfolio of effects…” Translation: empagliflozin and other medications from this class should be the second drug after metformin in diabetes treatment because it protects every cell and organ in the body by switching on AMPK. It is less about the sugar and more about molecular biology. Every green box intervention in the diagram directly or indirectly switches on AMPK and switches off mTOR. That is the key insight. That is the key to treating microvascular disease in our whole body and making women safer.
The evidence is in. The specific research on women with heart disease has been done. Now the challenge is to translate that research and scale it. OMT is the answer. It can be standardized, scaled, and industrialized. There are already primary care teams focused on urgent and hospital care. Chronic diseases generate over 80% of all healthcare costs. It is past time to develop primary case teams focused on chronic diseases who have continuing education to close the large gap between evidence and practice. The first 47 posts on this site beginning on January 1, 2021, provide the knowledge to get cardiometabolic teams on the same page so they consistently produce OMT.
Are we going to sit on our hands or are we going to do something? Get in touch if your institution, county, or town wants to start an OMT educational or treatment program. Women are dying while we figure this out.
This makes perfect sense! I’m champing at the bit to see my HCP provider next week to see what her thoughts are! Thank you Dr. B.
Spot on! Excellent follow up! Bill.