

Man With Recently Diagnosed Type 2 Diabetes Not on Metformin
Man With Recently Diagnosed Type 2 Diabetes Not on Metformin


This is another individual that I just recently discussed with our nurse coaching team. He is in his early 50s and was just diagnosed two years ago. He works in medicine and so he has some medical knowledge but knows that he needs to understand his disease better. He has been serious about his disease and has made good progress. His hemoglobin A1c was 10 and it is now 7.1. He has lost 8 pounds while dramatically improving his glucose control. Many times, the weight goes up with better control. His blood pressure is 110/74 which is also excellent. He is on lisinopril and a statin. If you are simply focused on controlling the pressure, sugar, and cholesterol, you would just pat this guy on the back and encourage him to keep up the good work. Getting these levels down is important, but the way you get them down is equally important.
He controls his sugar with Januvia and a sulfonylurea like glipizide. People with type 2 diabetes don’t die of high sugar. They die of heart attacks and strokes. Januvia and glipizide offer no protection against those catastrophes. He tried to take metformin but could not tolerate it because of diarrhea. His work sometimes required him to be away from a bathroom. This is a common reason that individuals stop metformin, but with proper instruction, most of them can take it. That is really important because taking metformin lowers the risk of a heart attack by 39% compared with other treatments that achieve the same sugar level.
If someone has diarrhea with metformin there is usually a way to get around it. Metformin comes in an immediate release and sustained released formulation. The immediate release floods the system with metformin all at once. That is much more likely to cause side effects. Take the sustained release tablets. Take them with the biggest meal of the day and increase the dose very slowly. The nurse and I discussed taking one 500 mg. sustained release tablet and cutting his glipizide in half. Glipizide increases insulin levels and metformin makes insulin work better. It would be possible to have a low blood sugar if we did not cut back on glipizide. Almost everyone can tolerate a single metformin tablet. The side effects are dose related. If the side effects are mild, they generally improve with time.
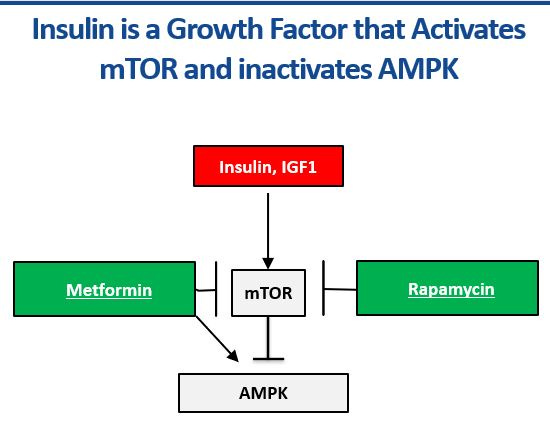
Why all the fuss about changing medicine. Look at the diagram above. Glyburide does not lower the risk of heart attack and stroke because it increases the insulin level. Insulin is important to control the sugar but too much insulin causes more heart attacks, strokes, and cancer. You want just enough insulin to control your sugar. Insulin causes problems because it does other things besides lowering your sugar. It is a growth factor that switches the master metabolic genetic switch mTOR on and it switches the master metabolic survival switch off. mTOR makes your heart bigger and your arteries thicker. It stimulates scar tissue to grow while killing the functional cells in the heart, kidney, and artery. mTOR makes you age faster and develop chronic diseases earlier. AMPK is a survival switch that protects all cells and organs. Metformin on the other hand directly inhibits mTOR while switching on AMPK. That is why getting on some dose of metformin is one of the most important goals in type 2 diabetes. Small doses of metformin that have a modest impact on glucose levels still switch off mTOR and switch on AMPK.
Lisinopril, losartan, eplerenone, and spironolactone for high blood pressure do the same thing. Our nurse coaches understand that and can improve clinical and financial outcomes.
Very important information, doctor.
💯%! That’s right.