

Optimal Medical Therapy is Much More Effective Than Usual Care
Optimal Medical Therapy is Much More Effective Than Usual Care

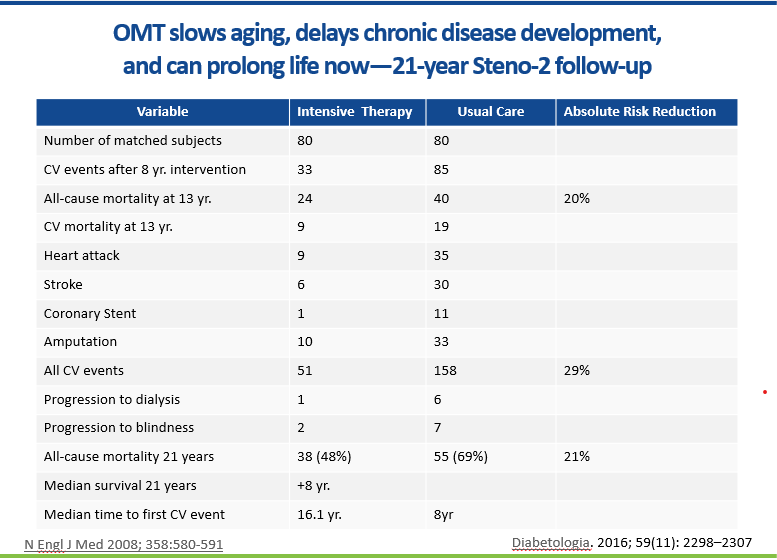
One out of four of us will die of heart disease. This slide comes from the Steno 2 trial which compared an intensive, multifactorial, protocol-driven, systematic intervention vs usual care in very high-risk patients with type 2 diabetes and chronic kidney disease.
Usual care is the care that most of us receive. The provider in usual care is on a hamster wheel. Her income depends on the number of office visits she produces per day. There is tremendouse pressure to keep moving. She is seeing all kinds of patients from individuals with a runny nose to patients with congestive heart failure who just left the hospital and are unstable. When she sees a patient like this, they have diabetes, hypertension, high cholesterol, and chronic kidney disease at baseline. That is four serious problems in a 15 minute visit. In addition, the patient most often has other problems like back pain and a rash that are their main concern. Those problem are new and take up most of the time in the visit. It is the chronic kidney disease that makes this person very high risk, but in this crazy system only 10% of Americans with chronic kidney disease even know they have it. Of course, if they don’t know they have it, they don’t know about their extreme risk and they are not engaged to protect themselves. The average age at enrollment in this study was 55. Half of these patients were dead by age 68. Everything depends on one person in this system—the provider. They must know: Did the patient have tests for kidney function this year; are those tests normal, do they understand the result? The provider is doing the best they can in a broken system.
Optimal medical therapy (OMT) is completely different. The practice has a focused primary care team with a physician, nurses, pharmacists, and medical assistants. The nurse and pharmacists have standing orders and computer tools to make certain that every patient has had the appropriate tests, medications, lifestyle advice, and they have achieved their goals. The usual care system is designed to generate office visits, referrals, and expensive tests. The intensive intervention in designed to solve a patient problem. It is patient-centered.
The main questions in OMT are different. The thought process is different too. The provider and patient in usual care are pushed and pulled by all kinds of controversy. What is the best initial drug for hypertension? How low should the blood pressure be? Are statins really that effective? Do they cause memory loss. The messages are extremely confusing and providers and patients are coming to very different conclusions.
In OMT, all team members are on the same page. The messages are consistent. There is a protocol with three targets and several interventions that apply to eighty to ninety percent of the patients. The blood pressure target is 130/80, LDL cholesterol 70 on a high-intensity statin, and sugar measure or hemoglobin A1c is 7. The team uses lisinopril or losartan, hydrochlorothiazide, amlodipine, and sprionolactone as needed to achieve the blood pressure goal. They make sure the patient is on high-intensity statin therapy, metformin for diabetes or prediabetes, and an aspirin. Every patient gets an eye exam, foot exam, and kidney testing annually. It is a comprehensive integrated systematic approach delivered by a special operations team designed for the task.
And there is just one more thing. There is a huge difference between anecdotes and evidence. Part of OMT is making certain that as many patients as possible are on the evidence-based treatments that make such a difference. Statin information is especially confusing and a perfect example of what I am talking about. In usual care, about half of the patients are on a statin and only about a quarter are on a high intensity statin. OMT teams achieve statin treatment rates of over 90%. Individual medications like statins may have modest effects and a few side effects, but when they are applied with lifestyle and other medications as listed above, the results attained are very diffent. The intensive group had 9 heart attacks and in usual care there were 35. The real question is this: what combination of lifestyle and medical treatments have the highest impact.
Anecdotes are a special problem. “My father took a statin and it made his memory worse.” Thousands of people are not taking statins because of stories like these. I have multiple cardiac risk factors and a documented 20% blockage of a heart artery. I take a high-intensity statin, I am 75 years old, and my memory for names is better than it was 5 years ago. The adverse memory impacts of statin therapy are temporary. The disappear when the medication is stopped. The memory impacts of stroke and vascular dementia are permanent. The memory problems with statin are greater early in treatment and lessen with duration of treatment. Memory actually improves in older patients on a statin. This is a great example of the damage done by anecdotes and testimonials and the critical role of evidence in patient care. The evidence supporting OMT as the standard of care are overwhelming. It is time to move!
This is amazing! I continue to ask myself..."Why don't we all do this and why do we not teach it in our various level medical education programs?" So sad that old ways die hard. :( And I appreciated your reference to the "hamster wheel" the other day. When I worked in a family medicine environment on a government installation that was absolutely the case. Thanks for your persistence in continuing to teach!
The one thing we must do is early detection and early warning to allow time for primary lifestyle optimization and OMT, if necessary, to reverse the cardiovascular disease progression and to dramatically reduce rate of untimely early deaths. Multifunction Cardiogram Technology delivers the early detection, early warning, and monitoring for disease reversal progress objectively, quantitatively, and timely at bedside at affordable costs.