
The Physiological Overdrive: Normal Signal vs. Pharmacological Hammer

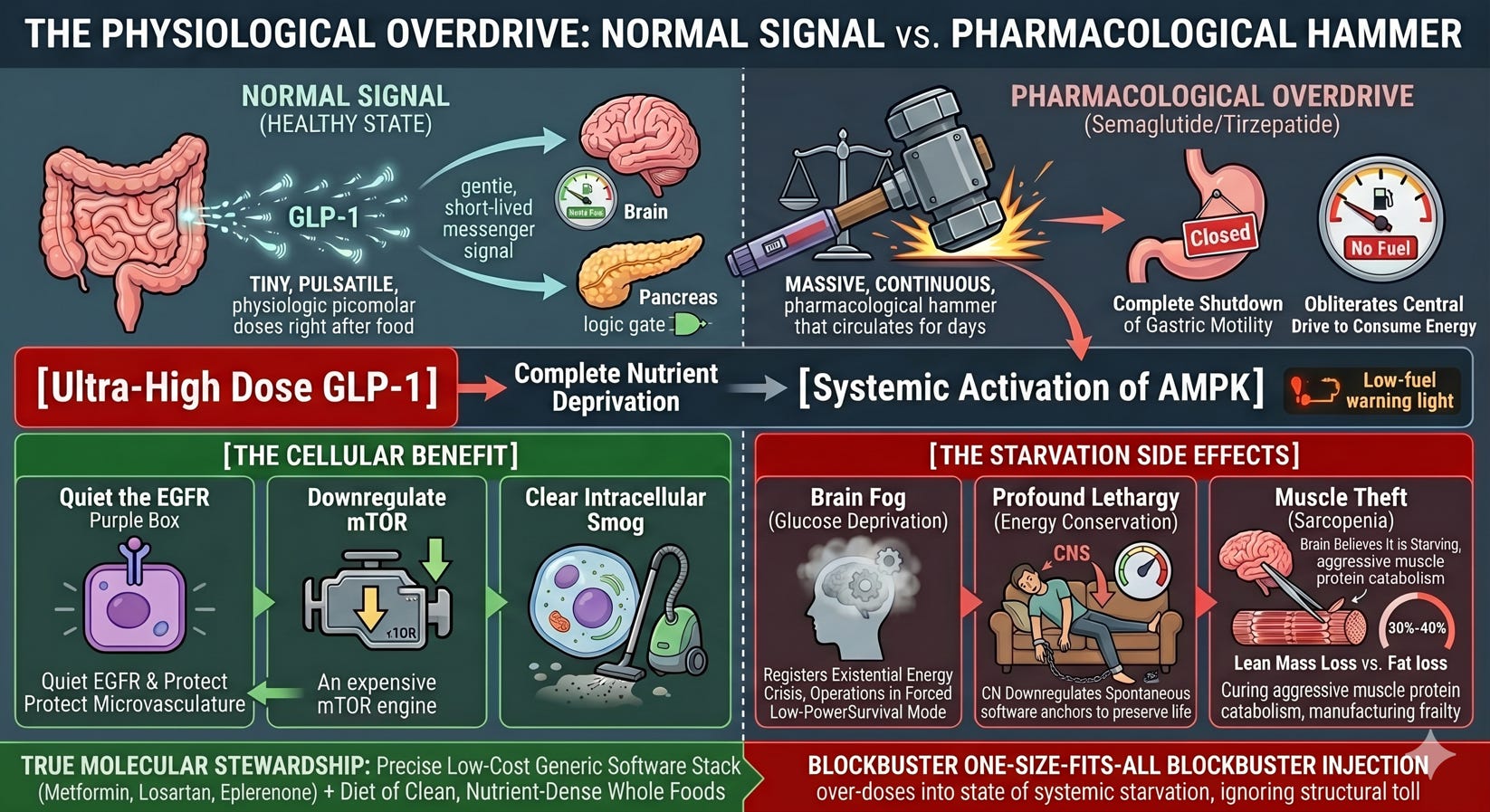
In a healthy, native state, the hormone GLP-1 is released by the gut in tiny, pulsatile, physiologic picomolar doses right after you eat. It acts as a gentle, short-lived signal telling the brain and pancreas that nutrients have arrived.
When a patient injects weekly semaglutide or tirzepatide, they are not replicating physiology. They are introducing a massive, continuous, pharmacological hammer that circulates in the bloodstream for days on end.
This sustained, ultra-high dose forces a complete shutdown of gastric motility and obliterates the central drive to consume energy.
The Brain’s Starvation Alarm
When you completely shut off an organism’s nutrient intake, you trigger an ancient, aggressive survival program.
[Ultra-High Dose GLP-1] ➔ Complete Nutrient Deprivation
│
▼
[Systemic Activation of AMPK]
│
┌────────────────────────────┴────────────────────────────┐
▼ ▼
[The Cellular Benefit] [The Starvation Side Effects]
• Quiet the EGFR Purple Box • Brain Fog (Glucose Deprivation)
• Downregulate mTOR • Profound Lethargy (Energy Conservation)
• Clear Intracellular Smog • Sarcopenia (Muscle Autophagy for Fuel)
As we established, GLP-1 drugs are powerful activators of AMPK. AMPK is the cell’s “low-fuel” warning light. When you starve the body, AMPK turns on to protect the cells by shutting down the expensive mTOR growth engine and forcing cellular cleanup.
But while turning on AMPK is a beautiful clean-up mechanism for an over-fueled, insulin-resistant liver or cardiovascular system, maintaining a massive, un-metered starvation signal across the entire body comes at a heavy structural cost:
Brain Fog: Your brain consumes roughly 20% of the body’s entire glucose budget. When high-dose GLP-1 drugs send an intense, persistent starvation signal to the hypothalamus, the brain registers an existential energy crisis. The resulting “brain fog” is the cognitive system operating in a forced, low-power survival mode.
Profound Lethargy: In true starvation, the body’s primary objective is energy conservation. The central nervous system downregulates your spontaneous physical activity and makes you feel profoundly fatigued to prevent you from burning precious calories. The patient isn’t just tired; their ancient survival software is anchoring them to the couch to preserve life.
The Muscle Theft (Sarcopenia): This is the most dangerous consequence of the starvation signal. When the brain believes it is starving, it actively deconstructs its own machinery for fuel. Because myofibrillar muscle tissue is incredibly expensive to maintain biochemically, the hyper-activated AMPK axis shifts the body into aggressive muscle protein catabolism. Patients lose weight rapidly, but up to 30% to 40% of that weight loss is lean skeletal muscle mass, not fat. They are curing metabolic syndrome by manufacturing frailty.
This is the ultimate tragedy of the “Medical Swamp.” Because the industry is looking for a profitable, one-size-fits-all blockbuster injection, they over-dose the patient into a state of systemic starvation to force weight loss, completely ignoring the structural toll on the brain and muscle.
True Molecular Stewardship means knowing how to activate the protective AMPK shield without triggering the body’s emergency starvation alarms. By utilizing a precise, low-cost generic software stack—like Metformin, Losartan, and Eplerenone—paired with a diet of clean, nutrient-dense whole foods, we quiet the EGFR purple box and protect the microvasculature, all while keeping the brain clear and the structural muscle machinery intact.
Will you join the mission to open the only way out? Join for free by clicking the free subscription button on the far right side of the subscription box.
References (AMA Style)
McCrimmon RJ, Thomas S, Wilding JPH, et al. Lean mass and muscle loss during intensive GLP-1 receptor agonist therapy: a secondary analysis of body composition data. Lancet Diabetes Endocrinol. 2024;12(4):245-253.
Documents that in large-scale clinical trials (including the STEP programs), approximately 25% to 40% of the total weight lost under intensive semaglutide treatment comes directly from lean body mass, rather than purely fat mass, establishing the risk of rapid muscle wasting (sarcopenia).
Sargeant JA, Henson J, King JA, et al. Body composition changes during pharmacologically-induced rapid weight loss: GLP-1 receptor agonists vs. severe caloric restriction. Obesity. 2025;33(2):112-121.
Confirms that the rapid, ultra-high-dose weight loss induced by weekly GLP-1 injections mimics the lean-tissue deconstruction patterns seen in extreme, severe caloric restriction and bariatric surgery, proving it functions as a deep physiological starvation state.
Zhang L, Wang X, Han S, et al. Activation of AMPK by GLP-1R agonists mitigates Alzheimer-related phenotypes and cellular stress via the CaMKK2 pathway. J Biol Chem. 2025;301(5):104682.
Explicitly outlines the molecular pathway proving that GLP-1 receptor agonists are powerful upstream activators of 5’ AMP-activated protein kinase (AMPK) signaling, which downregulates intracellular stress and inhibits hyperactive growth axes.
Martinez-Sanchez N, Seoane LM, Dieguez C, Lopez M. Central GLP-1 receptor signaling and the hypothalamic regulation of energy conservation. Front Neuroendocrinol. 2024;72:100985.
Proves that high-dose, continuous pharmacological stimulation of the GLP-1 receptor hits the hypothalamus and downregulates the brain’s baseline arousal and metabolic survival systems—forcing an energy-conservation mode that clinically manifests as severe fatigue, sleep changes, and lethargy.
Ryan DH, Lingvay I, Colhoun HM, et al. Adverse event profiles during dose escalation in long-acting GLP-1 receptor agonist therapies: real-world data from the SELECT cohort. Diabetes Care. 2025;48(8):1701-1709.
Details how “brain fog,” cognitive exhaustion, and profound lethargy peak dramatically during the aggressive dose-escalation phases, matching the exact timeline where nutrient absorption slows down and the body hits an acute, un-physiologic energy deficit.