
The Structural Barrier Bypassing Fragmented Silos via Fiduciary Mandate

1. The Core Scientific Reality
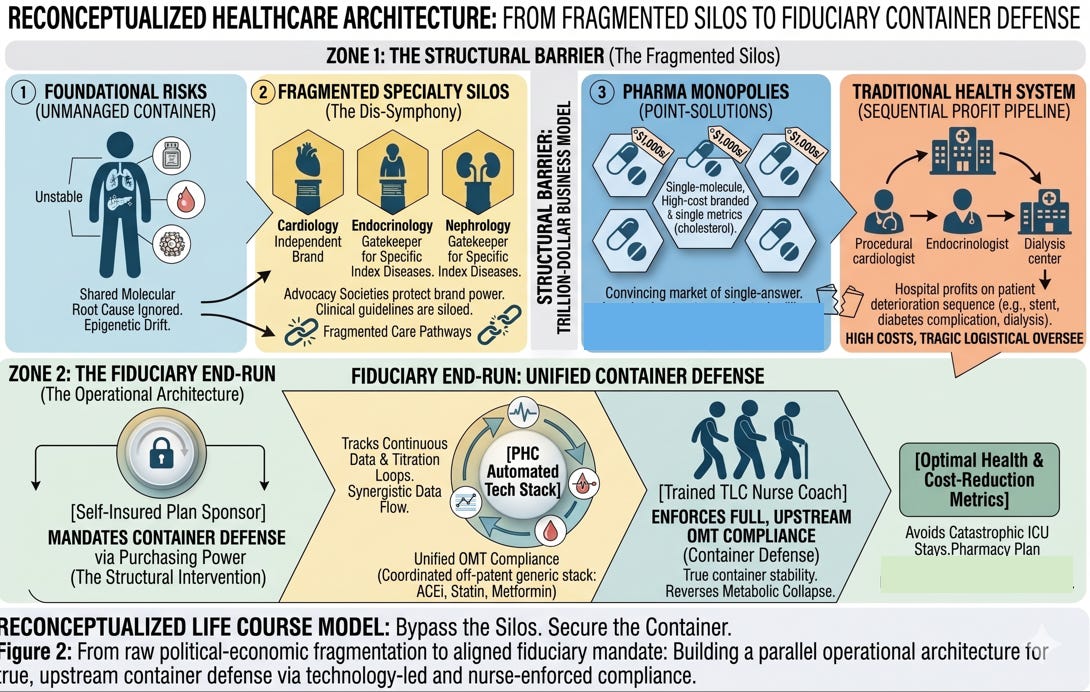
In its review of Cardiometabolic MLTC, The Lancet explicitly noted that fragmented, specialty-based care pathways are a primary barrier to patient survival and health system sustainability. However, our system continues to support this fragmentation to preserve their power, money, and influence in the face of overwhelming evidence that we must change our system to meet the needs of people with chronic diseases. .
As clinicians on the ground, we must understand the raw political-economic reality: this fragmentation is not an accidental flaw. It is an intentional, highly protected, and massively profitable business model.
The Advocacy Societies derive immense funding and institutional authority by acting as the exclusive gatekeepers for specific, index diseases. Admitting that these conditions share a singular molecular root cause dilutes their independent brand power and their control over clinical guidelines.
The Specialty Silos generate their highest margins when a patient deteriorates sequentially. A hospital system profits when a patient moves from a lucrative cardiology suite for a stent, to an endocrinology clinic, and finally to a high-volume nephrology center for dialysis. A unified protocol that stabilizes the entire container destroys the downstream procedural pipeline.
The Pharma Monopolies thrive on single-molecule, high-cost point-solutions. They do not profit from a $30-a-month coordinated stack of off-patent generics. They profit by convincing the market that a $1,000-a-month brand-name monopoly is the only acceptable answer to a single clinical metric.
The legacy medical-industrial complex is structurally incentivized to ignore systems-based medicine. They dug in and ignored the staggering 20% Absolute Risk Reduction mortality data from Steno-2 for two decades because keeping the container fragmented is a trillion-dollar enterprise.
2. The Clinical Application: The Fiduciary End-Run
Because the current clinical system is a structural barrier to progress, we cannot fix American healthcare by trying to change the minds of the legacy medical establishment. They will always dig in to protect their power and influence.
Instead, our model bypasses the traditional gatekeepers entirely by taking the clinical solution directly to the only stakeholder whose financial interests perfectly align with the patient’s underlying biology: the self-insured employer and plan sponsor.
The employer does not profit from a fragmented “dysymphony” of care. They bear the direct financial brunt of it:
They pay the $150,000 bills for catastrophic, unintercepted ICU stays.
They watch their pharmacy plans collapse under hyper-inflated branded point-solutions.
They suffer the devastating “Corporate Brain Drain” when chronic metabolic failure cuts down their most experienced senior leaders in their prime.
THE OPERATIONAL ARCHITECTURE
[ Self-Insured Plan Sponsor ] --> Mandates Container Defense via Purchasing Power.
│
▼
[ PHC Automated Tech Stack ] --> Tracks continuous data & titration loops.
│
▼
[ Trained TLC Nurse Coach ] --> Supports patients in OMT adherence and self-management.
By arming corporate fiduciaries and benefit brokers with The Lancet’s validation and real-world cost-reduction metrics, we empower employers to stage a structural intervention.
They use their purchasing power to bypass the unmanaged, siloed swamp entirely. They mandate a technology-backed, nurse-led support layer to deliver true, upstream whole body defense. We don’t wait for the establishment to reform its guidelines; we build a parallel operational architecture that leaves the legacy silos behind.
Will you join the mission to open the only way out? Join for free by clicking the free subscription button on the far right side of the subscription box.